Brain & Spine Care
Brain & Spine Care
Dr Tan Chi Chiu
Gastroenterologist

Source: Shutterstock
Gastroenterologist
If you are experiencing symptoms such as stomach pain or reflux, or if your doctor suspects a digestive disorder, you may be advised to undergo a gastrointestinal endoscopy. While this may sound intimidating, it's actually a non-surgical procedure that allows your doctor to examine your digestive tract and aid in the diagnosis of conditions like ulcers, celiac disease or even cancer.
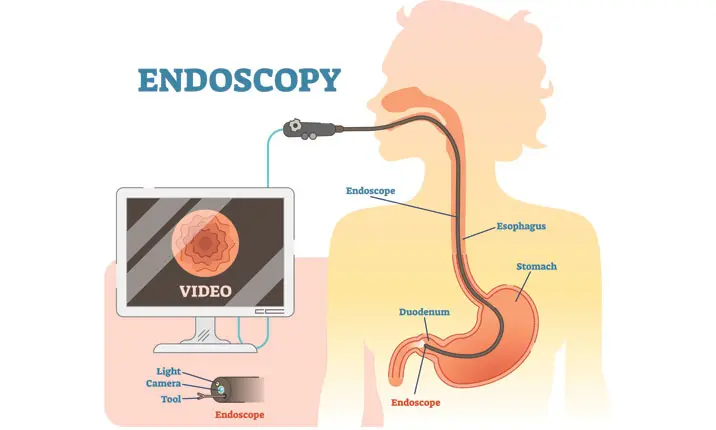
Gastrointestinal endoscopy involves the use of endoscopes. The endoscope is a thin, flexible tube fitted with a camera head and light guides. Designed with patient comfort in mind, this gentle device moves smoothly through your gastrointestinal tract to provide a clear picture of the insides of your oesophagus, stomach, duodenum and colon.
There are several types of endoscopy procedures, and each procedure is used to examine different parts of your digestive system.
A gastroscope examines your oesophagus, stomach and duodenum. The examination is called gastroscopy.
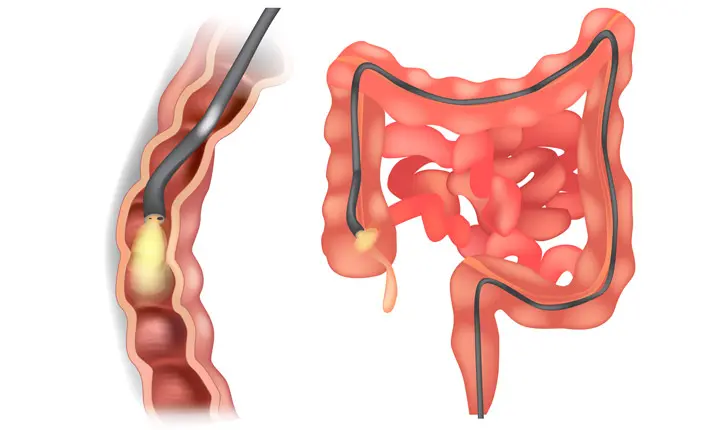
A colonoscope examines your large intestine or colon and can enter the last part of the small intestine (the ileum) that connects with the colon. If only a short examination is performed, it is called sigmoidoscopy. If a complete examination is done it is called colonoscopy.
A special kind of endoscope (ERCP side-viewing duodenoscope) allows visualisation and therapy of the bile ducts and pancreatic duct.
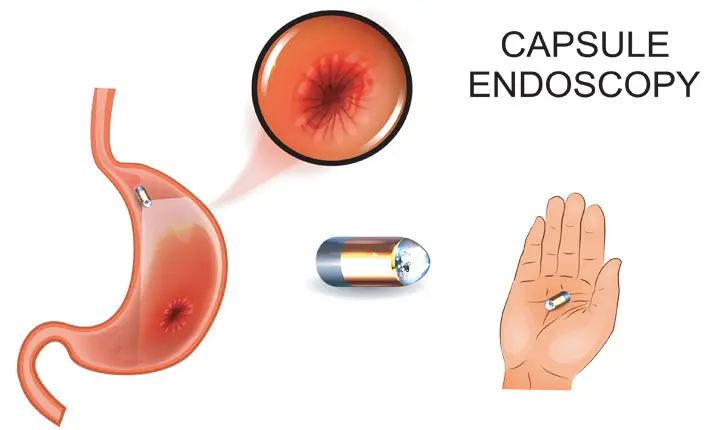
The small bowel can be visualised by modern methods such as capsule endoscopy or balloon enteroscopy.
Capsule endoscopy uses a high-tech capsule the size of a large vitamin pill, which contains camera, lights, lenses and a radio transmitting device. It is swallowed and as it moves through the small intestines, pictures are taken at a rate of two per second. The capsule transmits images to a recorder worn during the duration of the test and these thousands of images can be downloaded to a computer to be studied in detail. The capsule then passes harmlessly with the stools.
A balloon enteroscope is a modern endoscope that is fitted with a sheath with an inflatable balloon. By means of alternating inflation and deflation during advancement, the enteroscope can be advanced deeply into the small bowel, either through the upper or the lower digestive tract.
A power spiral enteroscope is another modern endoscope that is fitted with a powered spiral device that pleats the small bowel and advances the tip of the scope through the small bowel, either through the upper or lower digestive tract.
Endoscopic ultrasound (EUS) is performed by an endoscope with an ultrasound wave device at the head. This is used to examine the layers of the walls of the digestive tract and lesions in the wall, outside the wall or in organs adjacent to the digestive tract. For example, it is possible to examine cysts or tumours in the pancreas by doing EUS via the stomach wall.
A gastrointestinal endoscopy generally takes only 15 – 30 minutes. During this time, you may be sedated but general anaesthesia is usually not required. Many people fall asleep during this procedure.
As the endoscope is gently inserted into your body, true-to-colour high definition images are relayed electronically and displayed in real time on a monitor.
Modern endoscopes have a "narrow beam imaging" (NBI) function which changes the wavelength of the light used to examine the lining of the digestive tract and highlights abnormal features more clearly so that subtle abnormalities such as flat polyps can be detected. Other chromoendoscopy methods include dye sprays of the lining of the digestive tract to accentuate abnormalities.
Photographs and DVD recordings can be made for record purposes and given to the patient for future reference.
Results of endoscopy are known immediately and in many cases patients be offered initial treatment at once. If biopsies are taken, these results will be available after another one or two days.
A great advantage of endoscopy is that tiny surgical instruments can be passed through the endoscope to perform many functions. This includes taking biopsies, removing growths such as polyps, stopping bleeding from lesions, inserting stents (devices that hold open blocked tubes) and removing gallstones from the bile ducts.
A Nd-YAG laser or argon plasma fibre can also be passed down the endoscope to burn away cancers where appropriate or to coagulate bleeding blood vessels. In other imaging methods, including capsule endoscopy, the doctor can only see abnormalities but can do nothing to confirm diagnosis nor treat anything.
Not at all. Modern instruments are very thin and flexible and designed with patient comfort in mind. Patients undergoing gastroscopy and colonoscopy are also offered local anaesthesia by throat spray of lignocaine, as well as gentle sedation with intravenous injections of sedatives and analgesics, or a mild anaesthetic agent, carefully titrated to each individual patient's comfort. Patients are generally very comfortable throughout their procedures and usually awaken without any memory of having gone through them.
The sedation used in endoscopy is very gentle (unlike the general anaesthesia used in surgery), and there are minimal 'hangover' symptoms after awakening. In fact, most patients undergo endoscopy as day-cases and are in the Endoscopy Suite or Day Ward for only a few hours at most.
Patients who have morning procedures can, if they wish, return to work by the afternoon. Only in more complex cases will patients need to remain in hospital for a longer period for observation or further treatment.
For gastroscopy, capsule endoscopy, enteroscopy and examination of bile and pancreatic ducts, a patient only needs to fast for at least 8 hours prior to the examination, usually overnight, but can drink water if thirsty. This causes minimal inconvenience.
For colonoscopy, in order for the endoscopist to see clearly, a patient needs to take some gentle laxatives prior to the examination to clear the bowels of all stools. A few hours must be spent clearing the bowels and this can usually be done comfortably at home, or in the Endoscopy Centre.
All modern bowel preparation solutions are generally very easy to take and quite tolerable. Some patients find the taste a bit salty and need to drink plain water or a clear beverage such as 7-Up to cleanse the palate. If it is difficult to drink the bowel preparation solutions all at once, patients can sip it gradually instead. It is best to consume all the solutions prescribed to have the best chance of having a bowel that is clean enough for a thorough examination to be made.
Mental preparation is also important! Some patients have heard horror stories from friends or relatives, often from abroad, that an endoscopy was very uncomfortable because, in some places, endoscopy is performed without or with only minimal sedation. This may be due to lack of resources and time to titrate the sedative to the patient's comfort, or insufficient time to allow the patient to gently wake from the sedative before discharging them from the endoscopy unit.
However, in most modern practices, every effort is taken to ensure patients' comfort hence patients should not be worried about others' experiences as these may be in entirely different circumstances, and trust that their doctor aims to provide maximum comfort throughout the procedure.
While every precaution is taken to prevent complications during an endoscopy, there is still the possibility of risk. Known risks include:
Injury to the walls of the digestive tract is possible, with the worst case being a perforation that might require laparoscopic or key-hole surgery to repair. The risk is very small, especially in those with a relatively healthy digestive tract and an experienced endoscopist.
Medications to obtain conscious sedation may be given intravenously to help you relax and be comfortable during the procedure. This may cause vein irritation (phlebitis) or pain, an allergic reaction, or heart/breathing complications.
Bleeding may be a complication of biopsy, polypectomy, or dilatation and may rarely require blood transfusions or possibly a surgical operation. In diagnostic procedures, the risk of bleeding is virtually zero. The risk is higher if the polyp to be removed is large or if the procedure is complex.
Capped, loose, or false teeth or teeth in poor condition may be damaged during an endoscopy. Even normal teeth may be affected during safety or protective procedures relating to sedation, but this is rare. Although every effort is taken to protect patients' teeth, such damage is a recognised and accepted hazard of endoscopy.
This may be a result of ERCP, enteroscopy or endoscopic ultrasound with fine needle biopsy of a lesion or tumour of the pancreas.
Rarely, passage of the endoscope and manipulations may cause infection elsewhere in the body. However, transmission of infections between patients is virtually impossible due to extremely strict standards of sterilisation of the instruments employed.
You may experience sore throat, rectal irritation or abdominal bloating discomfort after an endoscopy. Air is often put into the stomach or colon to open it up for visualisation. While as much of this air as possible is removed at the end of the procedure, but there may still be some left behind. The air is usually easily passed and any discomfort will ease.
Endoscopy is an extremely effective means of examining the gastrointestinal tract, but it is not 100% accurate in diagnosis. Rarely, a failure of diagnosis or misdiagnosis may result, particularly with colonoscopy, due to the numerous turns and folds in the colon.
Although endoscopic ultrasonography is a valuable tool for the diagnosis of gastrointestinal, pancreatic and biliary conditions, a missed lesion such as cancer, can occur even in expert hands.
In spite of these, endoscopy is one of the most reliable methods of detection of gastroenterological diseases. Physical examinations, x-rays or other imaging techniques and laboratory tests can offer clues to health problems. But an endoscopy actually shows how your internal intestinal tissue looks, without surgery and with minimal risks and, where appropriate, treatment can even be provided through the endoscope.
If have any concerns or clarifications regarding a gastrointestinal endoscopy, please do not hesitate to contact your doctor, or check with your gastroenterology specialist to learn more about the procedure.

Dr Liau Kui Hin explains pancreatic neuroendocrine tumours (PNETs) and the newer, effective treatments for this uncommon cancer.

Inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS) can be difficult to differentiate. Dr Kelvin Thia explains.

Dr Dennis Chua talks about the thyroid and the common conditions associated with it.

The good news is that not all chest pain signals a heart problem. Dr Ooi Yau Wei explains the possible causes of chest pain and how to tell if the pain is heart-related.

When it comes to discussing more personal issues with doctors, it's tempting to hide certain details. Yet, by doing so, you may be putting your health at risk.

Can you tell if it is an acute or chronic injury? Learn how to distinguish between the 2 kinds, so you know how to get them treated.
Mount Elizabeth Hospitals are part of IHH Healthcare, one of the world’s largest integrated healthcare networks.
Download the MyHealth360 app to access an array of medical services conveniently.


Get trusted medical advice from our specialists, dietitians and physiotherapists directly in your inbox.
Subscribe