Brain & Spine Care
Brain & Spine Care
Dr Tan Chi Chiu
Gastroenterologist

Source: Shutterstock
Gastroenterologist
There are many causes of chest pain that can arise from the digestive tract, particularly in the oesophagus and the muscular tube that transports food from the mouth to the stomach.
Pain in the oesophagus can be felt in the centre of the chest, from the epigastrium (top of the soft part of the abdomen, below the breastbone) up to the throat. Oesophageal pain can also radiate to either side of the chest. When it radiates to the lower left part of the chest, the pain is sometimes misinterpreted as coming from the heart, such as during angina or a heart attack.
If you have concerns about your digestive health, speak to a specialist.
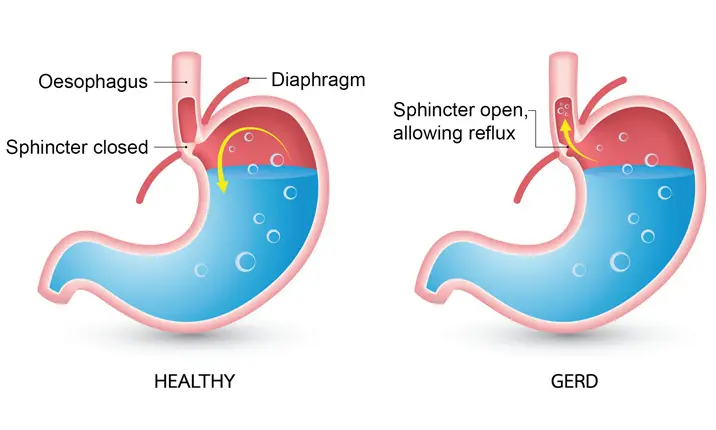
This digestive disorder is caused when excessive acid from the stomach, together with other caustic chemicals – such as the digestive enzyme pepsin and bile that refluxes into the stomach from the duodenum (early part of the small intestine) – flows back into the oesophagus. When these chemicals rise above the gastro-oesophageal junction (a physiological valve separating the oesophagus and stomach), they irritate and inflame the lining of the lower oesophagus.
The regurgitation of acidic stomach can cause a sore throat and leave a sour taste in the mouth. It could also damage the lower oesophagus, ranging from redness or mild inflammation to severe erosions and ulcerations, bleeding and scarring with stricture (tightening) of the oesophagus. This can lead to difficulties swallowing difficulties and pain.
Eosinophilic esophagitis, a variant of GERD, is an inflammation of the oesophagus that is thought to be related to allergies to various food groups or other environmental allergens. As part of the body's allergic reaction, white blood cells known as eosinophils infiltrate the lining of the oesophagus.
Chest pain due to gastric and other digestive problems can cause odynophagia, or painful swallowing. Gastric chest pain can be a sign of underlying oesophageal conditions, such as:
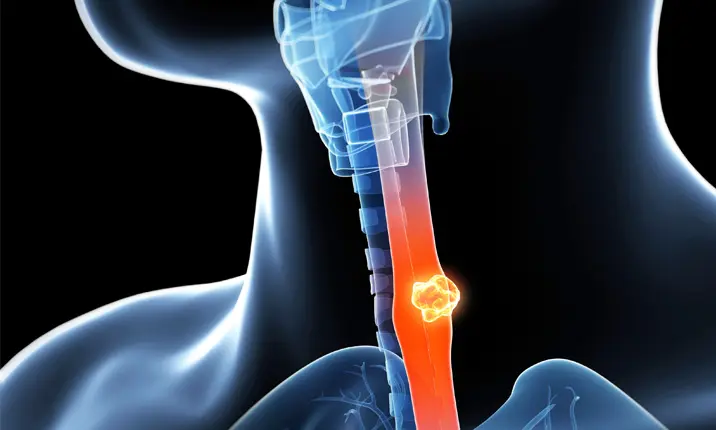
Cancer can develop in the squamous cells of the upper and mid oesophagus or the columnar epithelial cells of the lower oesophagus, adjacent with the stomach lining. The former, which is related to smoking and drinking scalding liquids, is becoming less common. On the other hand, the latter, which is related to acid reflux and smoking, is becoming more common.
In cancer which grows larger over time, the difficulty in swallowing, or dysphagia, is progressive. At first, it is difficult to swallow large, hard pieces of food, and eventually, even drinking water can become impossible.
Stomach cancer can block the entry of food into the stomach. When food backs up into the oesophagus, the pressure can cause pain in the chest.
As noted above, the oesophagus can narrow either due to swelling of the lining (EoE) or scarring by severe acid reflux. Food that is stuck in the oesophagus can also cause pain.
Motility is a term used to describe the contraction of muscles in the gastrointestinal tract. Motility disorders such as 'diffuse oesophageal spasm' or 'nutcracker oesophagus' cause strong disorganised contractions in the oesophagus that make swallowing difficult and painful.
A less common motility disorder is achalasia, a condition in which the muscles in the lower part of the oesophagus fails to relax to allow food to pass through as you swallow. Achalasia may occur in childhood or in adults. Some people are born with it while others develop the condition when another disease damages the nerves inside their oesophagus.
Also rare are oesophageal rings or webs – tissue growths which can develop in the upper or lower oesophagus. This often occurs from birth but is sometimes associated with reflux or iron deficiency anaemia. Plummer-Vinson syndrome or Paterson-Kelly syndrome often presents with a triad of symptoms – iron deficiency anaemia, dysphagia or difficulty swallowing, and an oesophageal web, which can be seen on a barium swallow test (an imaging test that uses x-rays to examine your upper gastrointestinal tract).
These medicines, such as Ibuprofen, can injure the lining of the entire digestive tract and cause inflammation in the oesophagus.
Some drugs may also become wedged in the oesophagus if not swallowed properly. Common culprits include potassium tablets, large multivitamin pills, and acne medication such as tetracycline and doxycycline. If you swallow pills lying down or fail to drink enough water with the medicine, caustic chemicals in the drugs can injure the oesophagus. In such cases, chest pain usually sets in several hours after taking the medication. Should the doctor conduct an endoscopy, circumferential ulcers can be found in the mid to lower oesophagus where the pill was lodged.
Children may swallow toys or other objects, while adults sometimes also inadvertently swallow foreign objects like toothpicks. (This can happen if you neglect to remove the toothpick in a cocktail snack and swallow it quickly – often in a semi-drunken state!)
Oesophageal infections are uncommon and more likely occur to in people with compromised immune systems, such as those who have diabetes mellitus, HIV, or are taking immunosuppressive drugs for other conditions. Infections caused by yeast (candida) or herpes viruses can also cause inflammation in the oesophagus result in a lot of pain.
As a general rule, chest pain that is severe, persistent or both, should receive medical attention so that a cardiac cause, such as a heart attack, can be quickly treated or eliminated.
If chest pain is mild, related to food and easily relieved by taking antacids (medication that neutralises stomach acidity), it may be acid-mediated and there is no urgency.
However, if simple measures such as antacids do not provide relief, or if the pain becomes more severe or persistent, you should see a doctor soon. As a rule of thumb, the more severe the pain, the more urgent it is to see a doctor, or even go to an emergency room.
To find out if a digestive disorder is causing your chest pain, your gastroenterologist may conduct an endoscopy to examine your oesophagus, stomach or small intestine. It is a non-surgical procedure where an endoscope, a flexible tube with a light and camera attached to it, is passed through the mouth and throat into the oesophagus.
The advanced field of endoscopy today makes it possible to diagnose causes of upper digestive tract symptoms. If therapeutic measures are required, there are also many techniques readily available. For example, it is possible to dilate a narrowed part of the oesophagus, use a laser or Argon plasma beam to shave away local obstruction caused by oesophageal cancer, and use instruments to retrieve food or a foreign object lodged in the oesophagus.
To diagnose motility disorders where visual findings by endoscopy may not yield enough information, there are now sophisticated devices for measuring pressure in various parts of the oesophagus, acid reflux into the oesophagus, and the flow of fluids up the oesophagus. Analysing these measurements can give doctors insight into the type of motility disorder that is causing your symptoms.
To get to the bottom of your chest pain or digestive problems, make an appointment with a specialist.

Inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS) can be difficult to differentiate. Dr Kelvin Thia explains.

The good news is that not all chest pain signals a heart problem. Dr Ooi Yau Wei explains the possible causes of chest pain and how to tell if the pain is heart-related.

Is your chest pain a heart problem? Find out what is causing your chest pain, and how to tell when it's serious.

Suffering from that familiar burning pain in your chest more than twice a week? Dr Poh Choo Hean explains what may be causing your pain.

The number of people with IBD has risen sharply in Asia and Singapore over the past few decades. Learn about your options to manage and treat IBD.

Irritable bowel syndrome is a pain in the gut (literally). But living with it doesn't have to be. Read our guide to understand more about IBS, and how you can manage it for a happy and healthy life.
Mount Elizabeth Hospitals are part of IHH Healthcare, one of the world’s largest integrated healthcare networks.
Download the MyHealth360 app to access an array of medical services conveniently.


Get trusted medical advice from our specialists, dietitians and physiotherapists directly in your inbox.
Subscribe